Our 33 organizations, representing the interests of the millions of patients and consumers who live with serious, acute, and chronic conditions, have worked together for many months to ensure that patient voices are reflected in the ongoing Congressional debate regarding the accessibility of health coverage for all Americans and families. In March 2017, we identified three overarching principles to guide and measure any work to further reform and improve the nation’s health insurance system. Our core principles are that health care must be adequate, affordable, and accessible. Together, our organizations understand what individuals and families need to prevent disease, manage health, and cure illness. Individuals and families with pre-existing conditions rely on critical protections in current law to help them access comprehensive, affordable health coverage that meets their medical needs. Unfortunately, the arguments of the plaintiffs in Texas v. U.S. – a lawsuit brought by 20 states and two individual plaintiffs – represent a serious threat to these protections. In this case, the plaintiffs argue that the court must invalidate the entire Affordable Care Act (ACA) due to Congress’ repeal of the individual mandate. We are further troubled that the Department of Justice has also declined to defend the constitutionality of many of the ACA provisions that directly protect people with pre-existing conditions.
Individuals and families with pre-existing conditions rely on critical protections in current law to help them access comprehensive, affordable health coverage that meets their medical needs. Unfortunately, the arguments of the plaintiffs in Texas v. U.S. – a lawsuit brought by 20 states and two individual plaintiffs – represent a serious threat to these protections. In this case, the plaintiffs argue that the court must invalidate the entire Affordable Care Act (ACA) due to Congress’ repeal of the individual mandate. We are further troubled that the Department of Justice has also declined to defend the constitutionality of many of the ACA provisions that directly protect people with pre-existing conditions.
 While we are pleased to see that you share our concerns about the potential impact of Texas v. U.S. on people with pre-existing conditions, as evidenced by your recent introduction of the Ensuring Coverage for Patients with Pre-Existing Conditions Act (S.3388), the safeguards presented in this legislation fall far short of the patient protections encompassed in existing law. This bill as written is far from an adequate replacement for the protections for individuals with pre-existing conditions that are provided under current law.
While we are pleased to see that you share our concerns about the potential impact of Texas v. U.S. on people with pre-existing conditions, as evidenced by your recent introduction of the Ensuring Coverage for Patients with Pre-Existing Conditions Act (S.3388), the safeguards presented in this legislation fall far short of the patient protections encompassed in existing law. This bill as written is far from an adequate replacement for the protections for individuals with pre-existing conditions that are provided under current law.
Current law requires issuers to comply with a set of provisions which work together to promote adequate, affordable, and accessible coverage for people with pre-existing conditions. Specifically, community rating, guaranteed issue, essential health benefits, cost-sharing limits, and the ban on pre-existing condition exclusions protect people with serious health care needs from discriminatory coverage practices. These policies are inextricably linked and removing any of them threatens access to critical care for people with life-threatening, disabling, chronic, or serious health care needs.
Adequacy
Health care must be adequate, covering the services and treatments patients need, including patients with unique and complex health care needs. It is paramount that protections including the Essential Health Benefit (EHB) requirement, the ban on annual and lifetime caps, caps on out-of-pocket costs, and restrictions on premium rating be preserved in all health care plans to which they currently apply.
We were particularly disappointed that S. 3388 fails to include an outright ban on pre-existing condition exclusions. While a consumer with pre-existing conditions can gain coverage, the bill would allow issuers to underwrite plans to exclude any type of care based on medical history or health status. For example, under S. 3388 a patient with a history of cancer may be able to gain coverage, but an issuer would still be allowed to exclude coverage for screenings or treatment for a reoccurrence. Continuing to allow issuers to sell plans that undermine access to comprehensive coverage directly contradicts the presumed intent of this legislation, puts consumers at risk for catastrophic healthcare costs or being forced to delay care, and creates additional confusion for consumers and patients.
Affordability
Our second principle recognizes that illness and disease impacts individuals across the economic spectrum. We believe that everyone – regardless of their economic situation – should be able to obtain the treatment they need to manage, maintain, or improve their health. This means that coverage should be affordable, including reasonable premiums and cost-sharing, and that individuals with pre-existing conditions should be protected from being charged more for their coverage.
Although this legislation protects against higher rates based on health status, we remain concerned that it leaves patients and consumers exposed to higher premiums based on other factors that can be used as proxies for health status, such as age, gender, or occupation. For instance, there is no limit on how much more insurers in the individual market could charge a 50-year-old with heart disease because of his age. Insurers could also charge higher rates to a woman of childbearing age because of her gender. This legislation would exacerbate the affordability challenges facing many Americans today by neglecting to maintain current protections and subjecting patients to even higher premiums should the ACA be completely invalidated.
Accessibility
Lastly, health care coverage must be accessible. All people, regardless of employment, health status or geographic location, should be able to gain coverage without waiting periods or undue barriers to coverage. While we appreciate that the legislation would continue to prohibit insurers from denying coverage to individuals with pre-existing conditions, we are deeply troubled that, absent other quality and financial protection standards, this provision would offer only minimal assurance to consumers.
Conclusion
While we do not yet know the outcome or scope of the ruling in the Texas v U.S. case, failure to preserve key ACA provisions could have catastrophic implications for both the insurance markets and the millions of patients who rely on them. Partially restoring only two (guaranteed issue and some rating protections) of the multiple provisions that currently protect patients is inadequate and would leave many people without the level of coverage they need and deserve. Should the ACA be struck down and this legislation implemented as a replacement, consumers with pre-existing conditions would face significant financial and coverage barriers. In short, for people with pre-existing conditions, the bill would provide access to coverage in name only.
We share your interest in continuing to make health insurance accessible to Americans with pre-existing conditions and appreciate your efforts to preserve certain protections in law, regardless of the outcome of Texas vs. US. However, the “Ensuring Coverage for Patients with Pre-Existing Conditions Act” as currently drafted, falls far short of providing coverage and security to your constituents, including those who are or will face significant health care needs. We urge you and your Senate colleagues to reconsider your approach to S. 3388 and ensure that any future legislation provides protections for people with pre-existing conditions that are the same or better than those included in current law.
Our organizations stand ready to work with you on solutions that serve the patients we represent and would be pleased to meet with you about how this legislation can be improved to meet the needs of people with pre-existing conditions.
___________________________________
This is the complete text of correspondence sent on September 19, 2018 to 16 members of the U.S. Senate, on behalf of 33 organizations including Danbury-headquartered National Organization for Rare Disorders (NORD) and many others with active chapters in Connecticut. Signatories also included Adult Congenital Heart Association, Alpha-1 Foundation, ALS Association, American Cancer Society Cancer Action Network, American Diabetes Association, American Heart Association, American Liver Foundation, American Lung Association, Arthritis Foundation, Chronic Disease Coalition, COPD Foundation, Crohn’s & Colitis Foundation, Cystic Fibrosis Foundation, Epilepsy Foundation, Family Voices, Global Healthy Living Foundation, Hemophilia Federation of America, Leukemia & Lymphoma Foundation, Lutheran Services in America, March of Dimes, Mended Little Hearts, Muscular Dystrophy Association, National Alliance on Mental Illness, National Coalition for Cancer Survivorship, National Health Council, National Hemophilia Foundation, National Kidney Foundation, National Multiple Sclerosis Society, National Patient Advocate Foundation, Susan G. Komen, United Way Worldwide, and WomenHeart: The National Coalition for Women with Heart Disease.




 More than 250 attendees are anticipated, to include consultants, coaches, funders, academics, and executives from across the country. The conference intends to “convene the diverse perspectives that shape and advance our field.”
More than 250 attendees are anticipated, to include consultants, coaches, funders, academics, and executives from across the country. The conference intends to “convene the diverse perspectives that shape and advance our field.”
 These numbers are high, but they correspond to previous research showing that on any given day, one-third of children consume fast-food… Furthermore, parents’ purchases of fast-food for their children increased significantly during the years examined, with parents reporting increased frequency of visits to most individual fast-food restaurants from 2013 to 2016…
These numbers are high, but they correspond to previous research showing that on any given day, one-third of children consume fast-food… Furthermore, parents’ purchases of fast-food for their children increased significantly during the years examined, with parents reporting increased frequency of visits to most individual fast-food restaurants from 2013 to 2016…
 Unhealthy options, including main dishes, sides, and desserts, remain on kids’ meal menus at most restaurants, and purchases of a kids’ meal plus another menu item for their child have increased. Although future research is required to explain the reasons for these trends, they do indicate that restaurants’ voluntary pledges, as currently implemented, are unlikely to substantially reduce children’s fast-food consumption overall, or increase their selection of available healthier drink and side options.
Unhealthy options, including main dishes, sides, and desserts, remain on kids’ meal menus at most restaurants, and purchases of a kids’ meal plus another menu item for their child have increased. Although future research is required to explain the reasons for these trends, they do indicate that restaurants’ voluntary pledges, as currently implemented, are unlikely to substantially reduce children’s fast-food consumption overall, or increase their selection of available healthier drink and side options.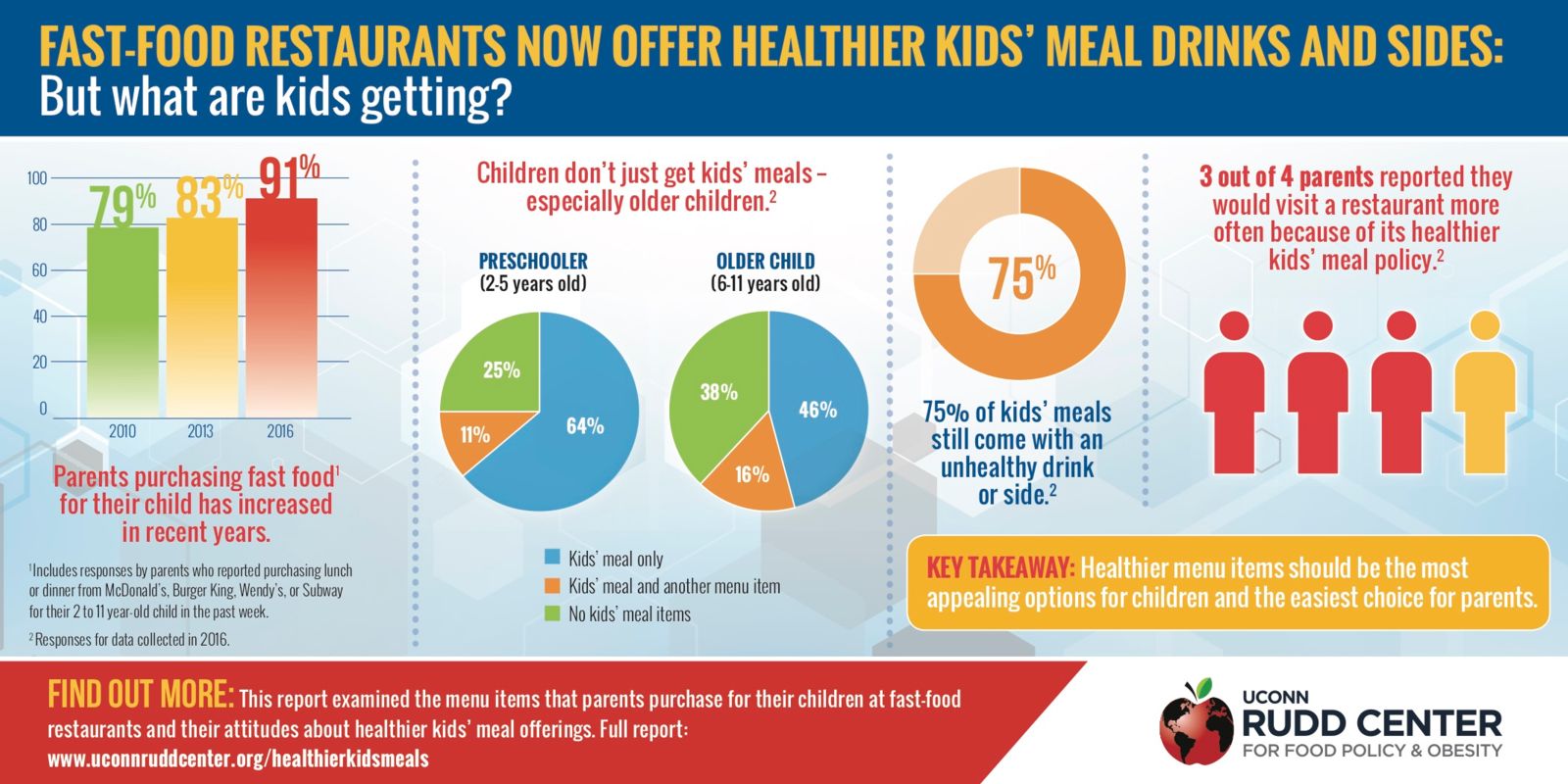
 e the community a better place.”
e the community a better place.”


 It went on to explain that “upon further look, there is a profound distinction among the projected population shift when broken down by age. Between 2010 and 2040, Connecticut’s age 65 years and over population is on pace to increase by 57%. However, its population between the ages of 20-64 is projected to grow less than 2% and the population age 18 and under is projected to decline by 7%.”
It went on to explain that “upon further look, there is a profound distinction among the projected population shift when broken down by age. Between 2010 and 2040, Connecticut’s age 65 years and over population is on pace to increase by 57%. However, its population between the ages of 20-64 is projected to grow less than 2% and the population age 18 and under is projected to decline by 7%.”
 Just over a decade later, her business acumen and history of public service put her on a ticket for statewide office. In 1990, New Haven-area Congressman Bruce Morrison won a primary to be the Democrats choice for Governor, former U.S. Senator Lowell Weicker started his own political party to launch is comeback with a candidacy for Governor, and Republicans nominated another Congressman, John Rowland of Waterbury.
Just over a decade later, her business acumen and history of public service put her on a ticket for statewide office. In 1990, New Haven-area Congressman Bruce Morrison won a primary to be the Democrats choice for Governor, former U.S. Senator Lowell Weicker started his own political party to launch is comeback with a candidacy for Governor, and Republicans nominated another Congressman, John Rowland of Waterbury.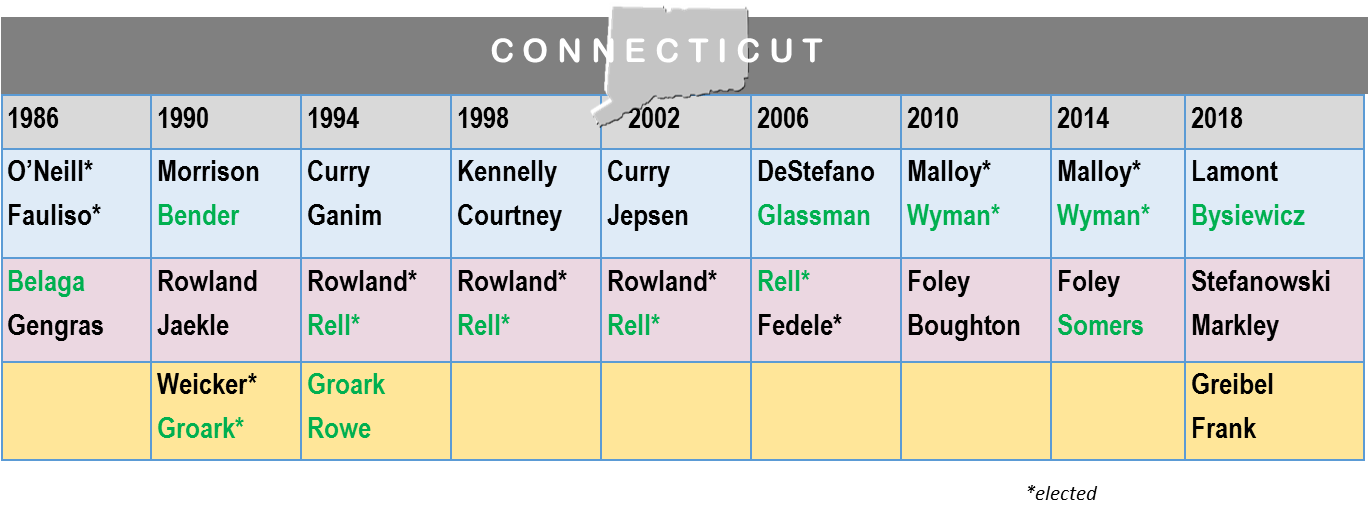
 She is also remembered as the Democratic candidate the first time two women were on the November ballot for Lieutenant Governor of Connecticut. That occurred again in 1994 and 2014. At least one woman has been a candidate for Lieutenant Governor or Governor - or both - in every election cycle since 1986, and Connecticut's voters elected Nancy Wyman to serve as Lieutenant Governor in 2010 and 2014, following one term of a man in that role, the only such term since 1990. This year, Susan Bysiewicz is on the ballot for that office. A woman has been elected either Governor or Lieutenant Governor in Connecticut in every election since 1990.
She is also remembered as the Democratic candidate the first time two women were on the November ballot for Lieutenant Governor of Connecticut. That occurred again in 1994 and 2014. At least one woman has been a candidate for Lieutenant Governor or Governor - or both - in every election cycle since 1986, and Connecticut's voters elected Nancy Wyman to serve as Lieutenant Governor in 2010 and 2014, following one term of a man in that role, the only such term since 1990. This year, Susan Bysiewicz is on the ballot for that office. A woman has been elected either Governor or Lieutenant Governor in Connecticut in every election since 1990.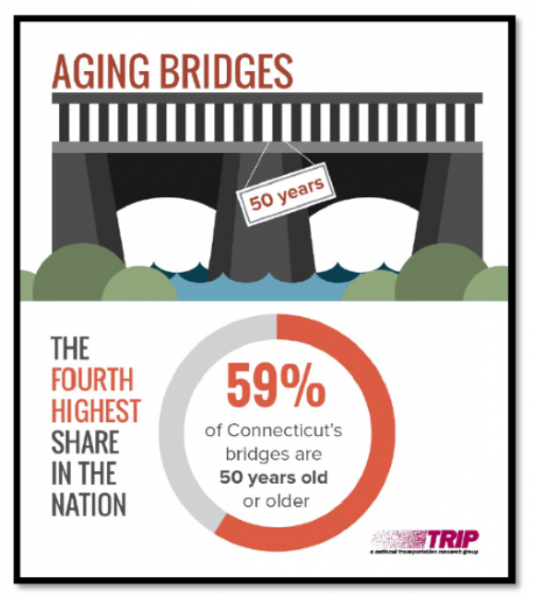 Yesterday, it was announced that 59 percent of Connecticut’s more than 4,000 bridges are 50 years or older, the fourth highest rate in the nation. The average age of all Connecticut’s bridges is 53 years, while the average age of the state’s 308 structurally deficient bridges – seven percent of the total - is 69 years. Structurally deficient bridges in Connecticut are crossed daily by 4.3 million vehicles.
Yesterday, it was announced that 59 percent of Connecticut’s more than 4,000 bridges are 50 years or older, the fourth highest rate in the nation. The average age of all Connecticut’s bridges is 53 years, while the average age of the state’s 308 structurally deficient bridges – seven percent of the total - is 69 years. Structurally deficient bridges in Connecticut are crossed daily by 4.3 million vehicles. The report also noted that “annually, $489 billion in goods are shipped to and from sites in Connecticut, largely by truck,” adding that “approximately 731,000 full-time jobs in Connecticut in key industries like tourism, retail sales, agriculture and manufacturing are completely dependent on the state’s transportation network.”
The report also noted that “annually, $489 billion in goods are shipped to and from sites in Connecticut, largely by truck,” adding that “approximately 731,000 full-time jobs in Connecticut in key industries like tourism, retail sales, agriculture and manufacturing are completely dependent on the state’s transportation network.”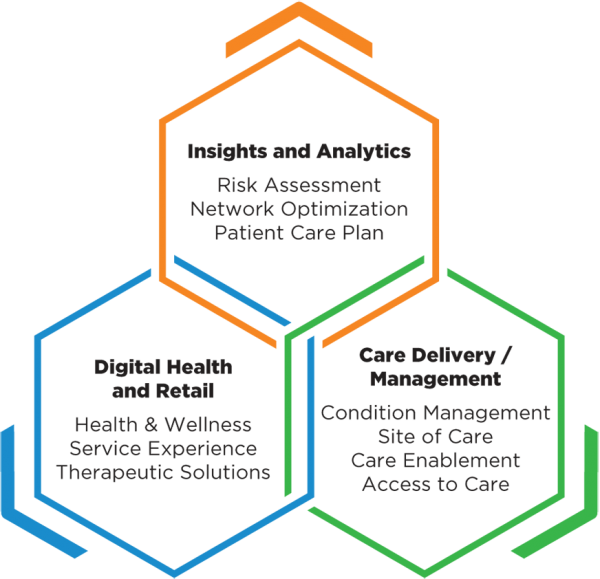 Companies in the portfolio, according to published reports, include Omada Health, a digital therapeutics company treating chronic diseases; Prognos, a predictive analytics company for healthcare; Contessa Health, a home-patient care service; Mdlive, which provides remote health consultations; and Cricket Health, a special kidney care provider.
Companies in the portfolio, according to published reports, include Omada Health, a digital therapeutics company treating chronic diseases; Prognos, a predictive analytics company for healthcare; Contessa Health, a home-patient care service; Mdlive, which provides remote health consultations; and Cricket Health, a special kidney care provider.

 Obesity is a problem in virtually every city and town, and every income and social sector. But its impact is most serious in communities where conditions make access to healthy foods and regular physical activity more difficult, such as lower income and rural areas, including many communities of color. The national costs of obesity are enormous, officials point out. Obesity drives an estimated $149 billion annually in directly related healthcare spending, and an additional $66 billion annually in lowered economic productivity. Also, one in three young adults is ineligible for military service, due to being overweight, officials noted.
Obesity is a problem in virtually every city and town, and every income and social sector. But its impact is most serious in communities where conditions make access to healthy foods and regular physical activity more difficult, such as lower income and rural areas, including many communities of color. The national costs of obesity are enormous, officials point out. Obesity drives an estimated $149 billion annually in directly related healthcare spending, and an additional $66 billion annually in lowered economic productivity. Also, one in three young adults is ineligible for military service, due to being overweight, officials noted.